



組織深達度が浅い 、優れた止血で安全かつ正確な手術を実現、患者様のQOLの向上に貢献
このサイトは、弊社が販売する製品に関する情報を、医療関係者の方に提供することを目的として作成されています。
一般の方への情報提供を目的としたものではありませんのでご了承ください。
あなたは医療従事者ですか?


レボリックス 200
ツリウム・ヤグレーザ
30200BZX00402000
組織深達度が浅い 、優れた止血で安全かつ正確な手術を実現、患者様のQOLの向上に貢献
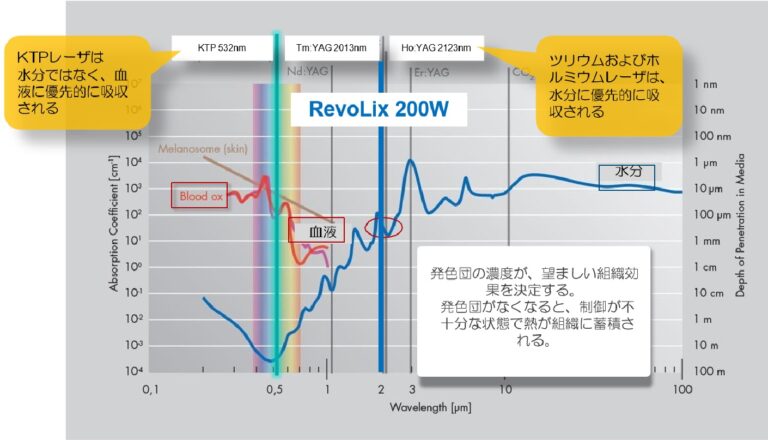
RevoLixのツリウムエネルギーは、ヒトの組織に高い割合で存在する水分に吸収され、正確な切除・凝固を実現
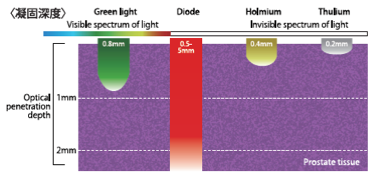
Table1: Optical penetration depth of different laser systems [28]
RevoLixツリウムヤグレーザは、KTPレーザと同様の止血特性を維持しながら、より高い組織切除能力を提供 [29]
ツリウムvs TURPに関するその他の出版物: Less short term complication rates: „The short-term
✓[Vaporization of the prostate] complication rate with Tm:YAG was […] less than that with TURP.“ [22]
✓Higher efficiency in tissue removal for Thulium-laser in comparison with TURP, shorter post- operative stay [27]
| ThuVAP | ThuVARP | ThuVEP | ThuLEP | ThuLEP in Oyster technique |
| hulium laser vaporisation of the prostate 2004 (Mattioli et al., 2008) | Thulium laser Vaporesection in Tangerine Technique TmLRP_TT 2005 (Xia, 2009) Vaporesection 2006 (Bach, Herrmann, Ganzer, Burchardt, & Gross, 2007) |
Thulium laser vapo‐enucleation of the prostate 2008 (Bach, Herrmann, et al., 2009) | ThuLEP Anatomical enucleation with Tm:YAG support +‐ mechanical tissue morcellator or mushroom 2009 (Herrmann et al., 2010) |
Tm:YAG Oyster Anatomical enucleation Oyster technique with Tm:YAG support and high power in situ vaporisation 2016 (Herrmann, 2016) |
| 手技 | 蒸散切除術 ThuVaRP | 蒸散術 ThuVaP | 蒸散核出術 ThuVEP | 鈍的核出術 ThuLEP |
| 概要 | 尿道前立腺部から小さな組織片に切除 | 尿道前立腺部から前立腺組織を蒸散 | 外科的皮膜付近の溝を蒸散させて腺(2葉または3葉技術)を核出 | 約100 Wのレーザ出力で中葉を除去。側葉はレゼクトスコープの機械的力を用いて押し出す。 |
| 出力設定 (W) | 90-200 | 120-200 | 90-120 | 90-120 |
| ファイバー | RigiFib 550
RigiFib 800 |
RigiFib 550
RigiFib 800 RigiFib 1000 |
RigiFib 550
RigiFib 800 |
RigiFib 550 |
| 治療可能な前立腺サイズ | >100 g | >120 g | 制限なし | 制限なし |
| 👍 | 短いラーニングカーブ 初期治療プロトコル |
短いラーニングカーブ モーセレーション不要 |
前立腺のサイズ制限なし 最良の臨床結果 |
前立腺のサイズ制限なし 前立腺の完全除去 |

最大で15回まで再使用可能でありコスト軽減を実現しなやかで折れにくい
1) Cui, D., Sun, F., Zhuo, J. et al. A randomized trial comparing thulium laser resection to standard transurethral resection of the prostate for symptomatic benign prostatic hyperplasia: four-year follow-up results. World J Urol 32, 683–689 (2014)
2) Xia S.J., Zhuo J., Sun X.W., Han B.M., Shao Y., Zhang Y.N.; “Thulium Lasers versus Standard Transurethral Resection of the Prostate: A Randomized Prospective Trial”; Eur Urol (2008) Jan. 53; 382-390
3) Wei H., Shao Y. Sun F., Sun X., Zhuo J., Zhao F., Han. B., Jiang J., Chen H., Xia S.; “Thulium laser resection versus plasma kinetic resection of prostates larger than 80 ml”; World J Urol (2014) 32; 1077-85
4) Yang Z., Wang X., Liu T.; “Thulium Laser Enucleation Versus Plasma kinetic Resection of the Prostate: A randomized Prospective Trial With 18 Month Follow-up”; Urol (2013) 82 (2); 396-401
5) Zhang F., Shao Q., Herrmann T.R.W.,Tian Y., Zhang Y.; “Thulium Laser Versus Holmium Laser Transurethral Enucleation of the Prostate: 18-Month Follow-up Data of a Single Center”; Urol (2012) 79 (4); 869-874
6) Herrmann T.R.W., Liatsikos E., Nagele U., Traxer O., Merseburger A.S., “EAU Guidelines on Laser Technologies”; Eur Urol (2012) 61 783–795
7) S2e Leitlinie “Therapie des Benignen Prostatasyndroms (BPS)”, 2014, DGU, AK BPS
8) Bach T., Xia S.J., Yang Y., Mattioli S., Watson G.M., Gross A.J., Herrmann T.R.W.; “Thulium:YAG 2 micron cw laser prostatectomy: where do we stand?”; World J Urol 28.2 (2010): 163-168
9) Hauser S., Rogenhofer S., Ellinger J., Strunk T., Müller S.C., Fechner G., “Thulium Laser (RevoLix) Vapoenucleation of the Prostate is a Safe Procedure in Patients with an Increased Risk of Hemorrhage”; Urol Int (2012) 88; 390-394
10) Bach T., Huck N., Wezel F., Häcker A., Gross A.J., Michel M.; “70 vs 120 W thulium:yttrium-aluminium- garnet 2 μm continuous-wave laser for the treatment of benign prostatic hyperplasia: a systematic ex-vivo evalu- ation”; BJU international 106.3 (2010): 368-372
11) Wendt-Nordahl G., Huckele S., Honeck P., Alken P., Knoll T., Michel M., Häcker A., “Systematic Evaluation of a Recently Introduced 2-Micron Continuous Wave Thulium Laser for Vaporesection of the Prostate”; J of Endourol (2008) May 22 (5); 1041-1045
12) Netsch C., Bach T., Herrmann T.R.W., Neubauer O., Gross A.J., “Evaluation of the learning curve for Thulium VapoEnucleation of the prostate (ThuVEP) using a mentor-based approach”; World J Urol, published online 24 June 2012
13) Teichmann H.-O., Herrmann T.R.W., Bach T.; “Technical Aspects of Lasers in Urology”; World J Urol, (2007),
14) Sun F., Han B., Cui D., Zhao F.,Sun X. Zhuo J., Jing Y., Liu H., Xia S., Yang Y., Luo G., Guo F.; “Long-term results of thulium laser resection of the prostate: a prospective study at multiple centers”; 2015 33, 503-508
15) EAU (European Association of Urology), Eds.; “Guidelines on Management of Non-Neurogenic Male Lower Urinary Tract Symptoms (LUTS), incl. Benign Prostatic Obstruction (BPO)”; Gravas S. (Chair), Bach T. , Bach- mann A., Drake M., Gacci M., Gratzke C., Madersbacher S., Mamoulakis C., Tikkinen K.A.O., Guidelines Associates: Karavitakis M., Malde S., Sakkalis V., Umbach R.; 2016 March
16) DeCao, H., Wang, J., Huang, Y., LiangLiu, R., JunLei, H., Gao, L., … & Dong, Q. (2015). “Comparison between thulium laser resection of prostate and transurethral plasma kinetic resection of prostate or transurethral resection of prostate” Scientific Reports, 5, 14542.
17) Peng, B., Wang, G. C., Zheng, J. H., Xia, S. Q., Geng, J., Che, J. P., … & Yang, B. (2013). “A comparative study of thulium laser resection of the prostate and bipolar transurethral plasma kinetic prostatectomy for treating benign prostatic hyperplasia” BJU international, 111(4), 633-637.
18) Yan, H., Ou, T. W., Chen, L., Wang, Q., Lan, F., Shen, P., … & Xu, J. J. (2013). “Thulium laser vaporesection versus standard transurethral resection of the prostate: a randomized trial with transpulmonary thermodilution hemodynamic monitoring” Intl J Urol, 20(5), 507-512.
19) Si, J., Gu, B., Chen, Z., & Fu, Q. (2016). “The RevoLix™ 2 μm Continuous Wave Laser Vaporesection for the Treatment of Benign Prostatic Hyperplasia: Five-Year Follow-Up” Photomedicine and laser surgery, 34(7), 297-299.
20) Gross, A. J., Netsch, C., Knipper, S., Hölzel, J., & Bach, T. (2013). Complications and early postoperative outcome in 1080 patients after thulium vapoenucleation of the prostate: results at a single institution. European urology, 63(5), 859-867.
21) Macchione, L., Mucciardi, G., Di Benedetto, A., Butticè, S., & Magno, C. (2013). Efficacy and safety of prostate vaporesection using a 120-W 2-μm continuous-wave Tm: YAG laser (RevoLix 2) in patients on continuous oral anticoagulant or antiplatelet therapy. International urology and nephrology, 45(6), 1545-1551.
22) Vargas, C., García-Larrosa, A., Capdevila, S., & Laborda, A. (2014). Vaporization of the prostate with 150-W thulium laser: complications with 6-month follow-up. Journal of endourology, 28(7), 841-845.
23) Yang, Z., Liu, T., & Wang, X. (2016). Comparison of thulium laser enucleation and plasmakinetic resection of the prostate in a randomized prospective trial with 5-year follow-up. Lasers in medical science, 31(9), 1797-1802.
24) Netsch, C., Stoehrer, M., Brüning, M., Gabuev, A., Bach, T., Herrmann, T. R. W., & Gross, A. J. (2014). Safety and effectiveness of Thulium VapoEnucleation of the prostate (ThuVEP) in patients on anticoagulant therapy. World journal of urology, 32(1), 165-172.
25) http://auanet.mediaroom.com/2018-05-17-AUA-Releases-New-Clinical-Guideline-for-Surgical-Management-of- Lower-Urinary-Tract-Symptoms-Attributed-to-Benign-Prostatic-Hyperplasia
26) American Urological Association. “Benign Prostatic Hyperplasia: Surgical Management of Benign Prostatic Hyperplasia/Lower Urinary Tract Symptoms” (2018, amended 2019) Guideline Statement 20
27) Bach, Thorsten, et al. “Prospective assessment of perioperative course in 2648 patients after surgical treatment of benign prostatic obstruction.” World journal of urology 35.2 (2017): 285-292.
28) Photoselective laser ablation of the prostate: a review of the current 2015 tissue ablation options
29) Wendt-Nordahl, Gunnar, et al. “Systematic Evaluation of a Recently Introduced 2-μm Continuous-Wave Thulium Laser for Vaporesection of the Prostate.” Journal of endourology 22.5 (2008): 1041-1046
[button_to_cart item=”item_001″ sku=”Thulium:YAG laser RevoLix 200W” value=”この製品の購入はこちら”]
| 文献名 | 著者 | アブストラクト |
| Retrospective Analysis of Short-Term Outcomes After Monopolar Versus Laser Endoscopic Enucleation of the Prostate: A Single Center Experience | Enikeev, MD, PhD, Petr Glybochko, MD, PhD, Zhamshid Okhunov, MD, Yuriy Alyaev, MD, PhD, Leonid Rapoport, MD, PhD, Dmitry Tsarichenko, MD, PhD, Mikhail Enikeev, MD, PhD, Nikolay Sorokin, MD, PhD, Alim Dymov, MD, PhD, and Mark Taratkin, MD |
Introduction: Endoscopic enucleation of the prostate(EEP) has been recognized as a viable treatment modality for men with benign prostatic hyperplasia (BPH). The aim of our study was to compare the efficacy and functional outcomes of three different techniques of EEP, including monopolar enucleation (MEP), holmium laser enucleation of the prostate (HoLEP), and thulium laser enucleation of the prostate(ThuLEP).
Methods: The study consisted of a retrospective comparison of pre-and postoperative parameters in men undergoing three types of EEP: MEP, HoLEP, nad ThuLEP. Functional parameters were evaluated before and 6 months after surgery, which included the International Prostate Symptom Score, maximum flow rate, postvoid residual volume, prostate volume, and sodium levels of all patients. Results: A total of 551 men with the mean age of 67.1 years were included in the study. Of these, MEP was performed on 95 patients, HoLEP was performed on 254 patients, and ThuLEP on 202 patients. The mean mass of morcellated tissue obtained during the three techniques did not differ significantly (p>0.05). Mean procedure times of ThuLEP and HoLEP were shorter than MEP demonstrating 72, 76, and 86 minutes, respectively (p<0.01). The mean catheterization time following laser EEPs was shorter than MEP as shown by 1.3, 1.3, and 3.8 days, respectively (p<0.01). Hospital stay times of HoLEP and ThuLEP were shorter than MEP demonstrated by 3.3, 3.4, and 6.9 days, respectively (p<0.01). Patients after MEP had significant decrease in postperative hemoglobin and sodium levels. All the groups showed statistically significant improvement in the aforementioned parameters following treatment. Conclusions: Both techniques of laser enucleation proved to be efficacious in the management of BPH. MEP of the prostate seems to be a highly promising addition to the list of enucleation techniques and was determined to be an effective and acceptable procedure, despite a higher complication rate. |
| 【タンジェリンテクニック】Long-term clinical study of Thulium laser resection of prostate-tangerine technique | Sun Feng,Ciu Di,Wei Hai-bin,Zhuo Jian,Han Ban-min,Zhao Fu-jun,Sun Xiao-wen… |
|
| 【蒸散核出】Long-term outcome following Thulium VapoEnucleation of the prostate | C. Netsch • A. Engbert • T. Bach • A. J. Gross |
|
| 【TURPとThuVaRPの比較】An Analytical Comparison of Short-term Effectiveness and Safety Between ThuliumYAG Laser | Joon Woo Kim, Yeon Joo Kim, Yoon Hyung Lee, Joon Beom Kwon, Sung Ryong Cho, Jae Soo Kim |
|
| 【ツリウムと電気メスの違い-80ml以上の前立腺に対して】Thulium laser resection versus plasmakinetic resection of prostates larger than 80ml ツリウムレーザによる切除と電気メスの切除の違い-80ml以上の前立腺に対して | Haibin Wei • Yi Shao • Feng Sun • Xiaowen Sun • Jian Zhuo • Fujun Zhao • Bangmin Han • Juntao Jiang • Huirong Chen • Shujie Xia |
|
| 【タンジェリンテクニックでの初期治療結果】Two-micrometer thulium laser resection of the prostate-tangerine technique for patients with acute urinary retention | Jian Zhuo & Hai-Bin Wei & Fu-Jun Zhao & Feng Sun & Bang-Min Han & Xiao-Wen Sun & Shu-jie Xia Bang-Min Han & Xiao-Wen Sun & Shu-jie Xia |
|
| EAUGuideline2011_24_Lasers and Technologies レーザー及び技術に関するガイドライン | Thomas R.W. Herrmann , Evangelos N. Liatsikos , Udo Nagele , Olivier Traxer , Axel S. Merseburger EAU Guidelines Panel on Lasers, Technologies |
Context: The European Association of Urology (EAU) Guidelines Office has set up a
guideline working panel to analyse the scientific evidence published in the world literature on lasers in urologic practice. Objective: Review the physical background and physiologic and technical aspects of the use of lasers in urology, as well as current clinical results from these new and evolving technologies, together with recommendations for the application of lasers in urology. The primary objective of this structured presentation of the current evidence base inthis area is to assist clinicians in making informed choices regarding the use of lasers in their practice. Evidence acquisition: Structured literature searches using an expert consultant were designed for each section of this document. Searches were carried out in the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, and Medline and Embase on the Dialog/DataStar platform. The controlled terminology of the respective databases was used, and both Medical Subject Headings and EMTREE were analysed for relevant entry terms. One Cochrane review was identified. Evidence synthesis: Depending on the date of publication, the evidence for different laser treatments is heterogeneous. The available evidence allows treatments to be classified as safe alternatives for the treatment of bladder outlet obstruction in different clinical scenarios, such as refractory urinary retention, anticoagulation, and antiplatelet medication. Laser treatment for bladder cancer should only be used in a clinical trial setting or for patients who are not suitable for conventional treatment due to comorbidities or other complications. For the treatment of urinary stones and retrograde endoureterotomy, lasers provide a standard tool to augment the endourologic procedure. Conclusions: In benign prostatic obstruction (BPO), laser vaporisation, resection, or enucleation are alternative treatment options. The standard treatment for BPO remains transurethral resection of the prostate for small to moderate size prostates and open prostatectomy for large prostates. Laser energy is an optimal treatment method for disintegrating urinary stones. The use of lasers to treat bladder tumours and in laparoscopy remains investigational.
欧州泌尿器学会(EAU)のガイドライン事務局は、泌尿器科分野のレーザに関して発表された世界の文献の科学的証拠を分析するという目的で、ガイドライン・ワーキング委員会を発足しました。この委員会は、ガイドラインを通じ、各分析結果の提示及び泌尿器科におけるレーザ技術の応用を提言する専門家により構成されています。ガイドラインには、臨床医にとって非常に参考になると委員会が考える、レーザの特性に関する情報も盛り込まれています。
本ガイドラインの目的は、技術的考慮事項についての情報提供、及び、他のEAU臓器別ガイドライン文書内容の、競争というより、補足にあります。 泌尿器科でのレーザ及び新しい技術の使用に関するこれらガイドラインは、物理的背景や生理学的及び技術的側面における情報を臨床医に提供すると同時に、進化する新技術の臨床初期結果を提示します。技術的ツールとヒトの組織、外科的側面と能力、そしてユーザーの利便性を含んだ、新しいツールの利点と欠点等の間に起こる相互作用に重点が置かれます、本ガイドラインにおいて委員会は、今後数年間でさらに拡大していくことを見込んで、レーザに焦点を当てました。 |
| ツリウムレーザ(RevoLix)前立腺蒸散核出術は、出血のリスクが高い患者における安全な治療法である | Stefan Hauser , Sebastian Rogenhofer, Jörg Ellinger, Timo Strunk, Stefan C. Muller, Guido Fechner |
目的:慢性抗凝固療法を受けている患者及び出血性疾患のある患者における、ツリウムヤグレーザ前立腺蒸散核出術(ThuVEP)の安全性とフィージビリティを評価する。
方法:慢性抗凝固療法を受けている患者及び出血性疾患のある患者における、ThuVEP治療の臨床データ(輸血率、ヘモグロビン変化、残尿、出血性合併症、合併症と残尿)をレトロスペクティブ分析(後ろ向き分析)した。抗凝固療法は手術中も中断しなかった。 結果:試験対象患者基準を満たす患者39人を特定した(慢性抗凝固療法を受けている患者32人、出血性疾患のある患者3人、両方に該当する患者4人)。平均ヘモグロビン量は術前12.9g/l、術後11.7g/lであった。輸血を受けた患者は1人。平均残尿量は術前166ml、術後47ml、術後36人の患者において自然発生的な排尿が可能であった。フォローアップ期間中、患者5人に肉眼的血尿があり、保守的に治療した。 結果:出血性疾患のある患者、又は、抗凝固薬や血小板凝集阻害薬を服用している患者において、ThuVEPは安全な治療法である。 |
| ツリウムレーザ前立腺核出術(ThuLEP): レーザを用いた解剖学的経尿道前立腺切除術 良性前立腺閉塞治療に新しい技術を導入 | Thomas R. W. Herrmann • T. Bach • F. Imkamp • A. Georgiou • M. Burchardt • M. Oelke • A. J. Gross |
背景 前立腺組織の経尿道的摘出は、良性の前立腺肥大および前立腺閉塞治療における一つの選択肢です。尿流動態結果は摘出組織の質量に直接的関係がありますが、術中・術後の羅患率とも直接関連しています。前立腺の経尿道的レーザ治療は、出血性合併症を減らしたり、出血性疾患のある患者や抗凝固薬を服用している患者でも治療できる等の利点があります。本文献の目的は、移行帯の経尿道的全摘出(核出術)にツリウムレーザを使用することで、副作用を最小限に抑えると同時に、尿流動態の有効性を最大にするという、今までにない解剖学的全核出の技術を発表することです。
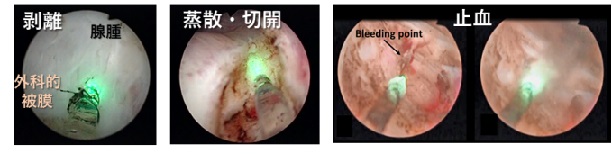
材料および方法 経尿道的前立腺移行帯全摘出術(ツリウムレーザ前立腺核出術、ThuLEP)における全く異なる5つの外科ステップを、術中画像と共に時系列に提示します。レーザエネルギーは、精丘および膀胱頸部で中葉を70~90Wで切開する時、また、側葉を切開する際、移行帯および膀胱頸部方向に外科的被膜を横切って流れる小血管を30Wで凝固させる時のみに使用します。葉部自体は、鈍的切開で遊離させます。 結論 ThuLEPは、前立腺の容積を問わず、移行帯を完全に摘出します。最大効果に最小副作用という利点を合わせ持つ技術です。ThuLEPを開腹前立腺切除術、または経尿道的切除術と比較する臨床結果が期待されます。 |
| Two micron continuous wave laser vaporesection for the treatment of benign prostatic hyperplasia | Wei-Jun Fu, Bao-Fa Hong, Yong Yang, Jiang-Ping Gao, Lei Zhang, Wei Cai, Yao-Fu Chen, Xiao-Xiong Wang |
I’m Wei-Jun Fu, from Department of Urology, Chinese
People’s Liberation Army General Hospital, Military Postgraduate Medical College, Beijing, China. We write to you to present an observation on the safety and clinical effects of RevoLix 70 W 2 micron continuous wave laser vaporesection for the treatment of obstructive benign prostatic hyperplasia (BPH). Because of the combination of the advantages of vaporization and resection,in our experience, 2 micron wave laser vaporesection for treatment of BPH provides safe and effective relief from obstructive BPH with minimal morbidity and rare bleeding. |
| Common trend: move to enucleation—Is there a case for GreenLight enucleation? Development and description of the technique | Fernando Gomez Sancha · Vanesa Cuadros Rivera · Georgi Georgiev · Alexander Botsevski · Julian Kotsev · Thomas Herrmann |
Background Transurethral laser prostatectomy has evolved as a viable alternative for the management of benign prostate enlargement. Since the renaissance of laser prostatectomy with the advent of the holmium:yttrium–aluminum– garnet laser in the 1990s, various lasers and subsequent
procedures have been introduced. These techniques can be categorized as vaporizing, resecting, and enucleating approaches. Photoselective vaporization of the prostate (PVP) is dominated by high-power lithium triborate (LBO) crystal lasers (GreenLight XPS). The mainstay of this technique is for the treatment of small to medium prostate volumes whereas enucleating techniques, such as holmium laser enucleation of the prostate and thulium enucleation of the prostate, focus on large-volume glands. In order to perspectively “delimit” LBO into the field of large-volume prostates, we developed LBO en bloc enucleation to render it as a competing transurethral enucleating approach. Materials and methods We present a detailed stepwise progressive technique developed in Madrid, Spain, for the complete removal of the transitional zone by vapoenucleation.The steps include exposition of the prostatic capsule by PVP toward the peripheral zone, thereby identifying the anatomical limits of enucleation. Subsequently, the transitional zone is excised in a single bloc and morcellated after its placement into the bladder. Conclusion This new GreenLight en bloc enucleation technique allows to treat larger prostates than those previously treated with the PVP technique. |
| Evaluation of the learning curve for Thulium VapoEnucleation of the prostate (ThuVEP) using a mentor-based approach | C. Netsch • T. Bach • T. R. W. Herrmann • O. Neubauer • A. J. Gross |
Introduction To evaluate the learning curve of Thulium:YAG VapoEnucleation of the prostate (ThuVEP) for patients with symptomatic benign prostatic obstruction (BPO) prospectively.
Methods ThuVEP was performed using the 120 Watt 2 lm continuous wave Thulium:YAG laser. ThuVEP was done by a resident without experience in transurethral prostate surgery (A, n = 32), an experienced endourologist (B, n = 32), and an experienced surgeon in ThuVEP (C, n = 32), who served as the mentor for A/B. Patients were divided into consecutive subgroups of 8 patients to assess the impact of the learning curve on procedure outcome. Patient demographic, perioperative, and 12-month follow-up data were analysed. Results ThuVEP was successfully completed in all patients. Enucleation efficiency (g/min) differed significantlybetween surgeon A (0.48 ± 0.3), B (0.7 ± 0.36),and C (1.4 ± 0.67) (p B 0.001). Enucleation efficiency correlated significantly with the weight of resected tissue in surgeon A (r = 0.88), B (r = 0.73), and C (r = 0.79) (p.001). ThuVEP was performed by surgeon A and B with reasonable enucleation, morcellation, and overall operation efficiency after 8–16 procedures. At 12-month follow-up, 68 (71 %) patients were available for review. IPSS, QoL, Qmax, PVR, PSA, and prostate volume improved significantly at follow-up (p B 0.023). Mean PSA/prostate volume reduction was 81.95/74.5, 80.7/79.4, and 87.6/75.9 % in surgeon A, B, and C, respectively. Urethral stricture and bladder neck contracture developed 2(A = 1, B = 1; 2.1 %) patients and 1 (C, 1 %) patient each, respectively. Conclusions ThuVEP can be performed with reasonable efficiency even during the initial learning course of the surgeon when closely mentored. Previous experience in the field of endourology is beneficial. |
| 文献名 | 著者 | アブストラクト |
| 腎細胞癌に対するレーザ腎部分切除術 | Torsten Gruschwitz, Renate Stein, Jörg Schubert, and Heiko Wunderlich |
目的 腎部分切除により、抹消にできた腎腫瘍を摘出する方法が、確立されております。血管肺門をクランプすることによる欠点を減らすために、腎部分切除にレーザを用いることを証明しました。現在のところ、このレーザの適用は、動物モデルにおいてのみ報告されています。
方法 腎腫瘍が腎臓の外側に増殖している患者のうち、私達は5名の患者において、腎血管をクランプすることなく、腎温存手術を行うことに成功しました。 結果 定期的な超音波モニタリングにおいて、術後出血を示す形跡はなく、手術前後の血清クレアチニン、ヘモグロビン、ヘマトクリット値に、ほとんど変化はありませんでした。 結論 私達の研究結果では、レーザによる腎部分切除は、慎重に選択した患者に対して、腎血管をクランプせずに適用可能であり、従来の腎部分切除に取って代わる安全な手技であることが示されました。 |
| 上部尿路における限局性上皮腫瘍の逆行性腎内手術に ツリウムレーザ・アブレーションを用いた最初の共同体験 | Lorenzo Defidio1, Mauro De Dominicis1, Luca Di Gianfrancesco1, Gerhard Fuchs2, Anup Patel3 |
目的:上部尿路移行上皮癌(UUT-TCC)の逆行性腎内手術(RIRS)における、ツリウムレーザ・アブレーション(TLA)結果と盲検性能評価の提示。
対象患者および研究方法:ヨーロッパの施設(2005年4月~2009年7月)での国際内視鏡手術共同プロジェクトにより、RIRS-TLAを受けたUUT-TCC患者のコホートを対象に、手術結果を評価しました。外科医4人は盲検にて、TLAおよびホルミウムヤグレーザ・アブレーションの性能的側面について個別に年1回、リッカート評価法(0-10)を用いて採点しました。 結果:すべての患者(n=59、年齢中央値66歳、単腎9人)がUUT検査を受け、その結果明らかとなった病巣は、腎内(n=30.51%)、尿管(n=13.22%)、混合(n=16.27%)でした。1回のTLAで成功(腫瘍根絶)したのは81.4%(腫瘍<1.5cm)でした。無再発生存率の違いは、原発腫瘍サイズ>/<1.5cmおよび多発性に応じて有意でしたが、部位による違いはありませんでした。リッカートスコア中央値はホルミウムヤグレーザおよびTLAでそれぞれ、i) ファイバーチップの安定性 -5.5/8.75、p=0.016*;ii) 出血量減少 -5/8.5、p=0.004*;iii) ファイバーチップの精度 -5.5/8.5、p=0.003*;iv) 粘膜穿孔減少 -3.5/7.5、p=0.001*;v) 切削効率 腫瘍<1.5cmの時 -6/9、p=0.017*;腫瘍>1.5cmの時 -6.75/6.75、p=1;vi) 全体効率 -6/7.5、p=0.09でした。 結論:UUT-TCCのRIRSにおける無再発生存率に関して、ツリウムレーザはホルミウムヤグレーザ・アブレーションに引けを取らない結果でしたが、ファイバーチップの安定性および精度、出血量減少、粘膜穿孔減少における専門家のパラメーター性能(中央値)評価は、より優れたものでした。腫瘍<1.5cmについては、光熱凝固および内部可視化が向上したにも拘らず、大きな腫瘍に対する切削効率および全体効率は、既存のレーザ技術では引き続いて厳しい状況でした。 |
| 尿道狭窄治療における経尿道的2µmレーザの適用 | Feng Fu Guo · Hua Lu · Guang Jian Wang · Shan Feng Tan · Xiang Fei He · Jian Ming Wang · Hong Jun Liu · Wen Bin Zhu |
目的 尿道狭窄治療に2µmツリウムレーザを用いた、経尿道的レーザ尿道切開術の治療効果を評価する。
方法 2µmツリウムレーザを使用した経尿道的レーザ尿道切開術を受けた、平均年齢47.3(36-58)歳の尿道狭窄男性患者238人に対して、術前、カテーテル抜去直後、術後3ヶ月および6ヶ月の各時点における最大尿流率(MFR)、国際前立腺症状スコア(IPSS)、生活の質アンケート結果(QoL)を測定しました。 結果 手術の際、すべての患者において直腸損傷、尿漏出、大量失血等の発生はありませんでした。カテーテル抜去後すぐに排尿も可能で、平均MFRは術前の3.2±0.3ml/sからカテーテル抜去後16.7±3.1に向上し、術後3ヶ月には18.7±2.9および6ヶ月には19.2±2.8と安定した数値を維持しました。IPSSは術前28.3±5.8から7.1±1.9、6.4±1.5、5.3±1.3[表の数値と違う]と各時点において顕著な向上を見せました。同期間のQoLも、各時点で5.4±1.1、1.1±0.3、0.9±0.2、0.8±0.2と向上を示しています。フォローアップ6ヶ月間、患者195人は再発せず、常時、連続排尿が可能となりました。患者43人は再発し、カテーテル抜去後7人に1-3週間(平均13.8日間)の失禁が見られましたが、定期的な尿道拡張と運動により、すべての患者が最終的に治癒しました。 結論 尿道狭窄における経尿道的2µmツリウムレーザの適用は、安全かつ有効です。 |
| 筋層非浸潤性膀胱癌の経尿道的レーザ治療における最新エビデンス | Mario W. Kramer • Thorsten Bach • Mathias Wolters • Florian Imkamp • Andreas J. Gross • Markus A. Kuczyk • Axel S. Merseburger • Thomas R. W. Herrmann |
はじめに
膀胱癌は、泌尿器系腫瘍で2番目に最も頻度の高い悪性腫瘍です。レーザが膀胱腫瘍治療のエンドウロロジー装備に加えられたのは、遡ること1976年のことです。筋層非浸潤性膀胱癌において、ワイヤループを介した経尿道的膀胱腫瘍切除(TRUB)による、最近の標準的病期診断や治療法があるにも拘らず、ホルミウムヤグレーザ(Ho:YAG)および、言うまでもありませんが、最新のツリウムヤグレーザ(Tm:YAG)の仲間入りで、膀胱腫瘍のレーザ切除術が再び脚光を浴びることになりました。本レビューは、これら技術の最新エビデンスを提示することを目的とします。 対象および方法 2010年4月を通して、MEDLINEとCochrane central register of controlled trialsを使い、以下のキーワードの検索をあらかじめ実施しました:レーザ、切除、アブレーション、凝固、Nd:YAGネオジム、Ho:YAGホルミウム、Tm:YAGツリウムおよび移行性癌、膀胱、膀胱内。 結果 Ho;YAGに関する文献が11件、Tm:YAGに関する文献が7件見つかりました。Cochrane online libraryでの検索で利用可能な資料はありませんでした。 結論 現在、下部尿路移行上皮癌の治療にNd:YAGは利用されていません。Ho;YAGとTm:YAGは膀胱癌治療にさまざまな選択肢を提供しそうですが、長期フォローアップの大規模ランダム化比較実証研究において、その可能性を示す必要があります。腫瘍の一括切除が、従来の「切開および散乱」切除法よりも好ましいかが(腫瘍学的外科原則すべてに反するところでありますが)、今後期待されるところです。ここでは、主要標的部位についての局部と局部外における低い再発率に加え、初回疾患除去の範囲内のデータを示します[本研究の主要目的は、局部と局部外における低い再発率に加え、初回で疾患を除去することです?]。 |
| 【腎癌治療における腎部分切除(ヒトへの摘要11人)虚血時間を短くする試み】 |
Background: To date, elective nephron-sparing surgery is an established method for the exstirpation of renal
tumors. While open partial nephrectomy remains the reference standard of the management of renal masses laparoscopic partial nephrectomy (LPN) continues to evolve. Conventional techniques include clamping the renal vessels risking ischaemic damage of the clamped organ. Thus, new techniques are needed that combine a |
|
| 腎細胞癌に 対する 虚血時間を 虚血時間を なくしたレーザによる レーザによる 腹腔鏡下腎部分切除 腹腔鏡下腎部分切除 | Hagen Loertzer*, Arne Straus, Rolf Herrmann Ringert and Philine Schneider |
背景 :現在のところ 現在のところ 現在のところ 、選択的 、選択的 、選択的 腎温存手術 腎温存手術 腎温存手術 が、 腎腫瘍 を摘出 する方法 する方法 する方法 として確立 として確立 として確立 されて されて います 。開腹腎 部分切除 部分切除 が腎腫瘤 を管理 する参考 する参考 基準 となっている一方で となっている一方で となっている一方で となっている一方で となっている一方で 、腹腔鏡下腎部分摘除術( 腹腔鏡下腎部分摘除術( 腹腔鏡下腎部分摘除術( 腹腔鏡下腎部分摘除術( 腹腔鏡下腎部分摘除術( 腹腔鏡下腎部分摘除術( LPNLPNLPN)が進化し ています ています 。従来 。従来 。従来 の方法 では、腎血管 をクランプ クランプ するため するため 、クランプ クランプ した臓器 した臓器 した臓器 が虚血性 虚血性 障害となる 障害となる 障害となる リス クがあった があった があった め、新しい 新しい LPNLPNLPNでは、 では、 腫瘍を 腫瘍を 摘出 する ための ための 十分な 十分な 組織切開 組織切開 と、 止血 を確実 を確実 にし 、腎 血管クランプを 血管クランプを 血管クランプを 不要にする 不要にする 不要にする 効率的な組織凝固を 効率的な組織凝固を 効率的な組織凝固を 効率的な組織凝固を 効率的な組織凝固を 兼ね備えた技術が 兼ね備えた技術が 兼ね備えた技術が 兼ね備えた技術が 必要 とされます とされます 。レーザ 。レーザ 。レーザ による による 腹腔 鏡下 腎腫瘍切除 腎腫瘍切除 腎腫瘍切除 は、 論理的 論理的 解決 法と考えられています と考えられています と考えられています と考えられています と考えられています 。
方法 :腎腫瘍 :腎腫瘍 :腎腫瘍 (平均 (平均 サイズ サイズ 32mm 32mm、範囲 、範囲 8~45 mm )が腎臓の外側に増殖している が腎臓の外側に増殖している が腎臓の外側に増殖している が腎臓の外側に増殖している が腎臓の外側に増殖している が腎臓の外側に増殖している が腎臓の外側に増殖している 患者 11 名に対し に対し て、腎血管 腎血管 をクラン クラン プする ことなく、レーザによプする ことなく、レーザによプする ことなく、レーザによプする ことなく、レーザによプする ことなく、レーザによプする ことなく、レーザによプする ことなく、レーザによLPN で、腎温存手術を で、腎温存手術を で、腎温存手術を で、腎温存手術を で、腎温存手術を 実施しまた。 実施しまた。 実施しまた。 結果 :定期的な 定期的な 定期的な 超音波 超音波 診断 、および および 一時的 一時的 に挿入した に挿入した に挿入した ドレナージ ドレナージ ドレナージ カテール カテール カテール において おいて 、術後の出血を 、術後の出血を 、術後の出血を 、術後の出血を 、術後の出血を 示す形跡は 示す形跡は あり ませんでした。 ませんでした。 ませんでした。 すべ ての腫瘍は の腫瘍は の腫瘍は 、病理組織学的に確認 、病理組織学的に確認 、病理組織学的に確認 、病理組織学的に確認 、病理組織学的に確認 された周囲の された周囲の された周囲の 正常な腎組織 正常な腎組織 正常な腎組織 正常な腎組織 の辺 縁ごと 摘出 しまた( しまた( しまた( R0 切除)。 切除)。 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 血清クレアチニン、ヘモグロビマトリッ値は手術前後 で、 ほとんど ほとんど ほとんど 変化はありませんでした。 変化はありませんでした。 変化はありませんでした。 変化はありませんでした。 変化はありませんでした。 変化はありませんでした。 結論 :今回 の研究結果 研究結果 研究結果 を通して 、レーザによる 、レーザによる 、レーザによる 、レーザによる LPNLPNLPNは、腎腫瘍が 腫瘍が 腎臓 の外側 に増殖している 増殖している 増殖している 増殖している 患者 に 対して、 対して、 腎血管を 腎血管を 腎血管を クランプ クランプ クランプ せずに せずに 適用可能であり、 適用可能であり、 適用可能であり、 適用可能であり、 適用可能であり、 従来 の腎部分切除 腎部分切除 腎部分切除 を代替する を代替する 安全で 安全で 低侵襲な 低侵襲な 低侵襲な 治療 法となり得る なり得る なり得る ことが ことが 確認 され ました。 ました。 |
| Current evidence for transurethral laser therapy of non-muscle invasive bladder cancer 膀胱がん | Mario W. Kramer • Thorsten Bach • Mathias Wolters • Florian Imkamp • Andreas J. Gross • Markus A. Kuczyk • Axel S. Merseburger • Thomas R. W. Herrmann |
Introduction Bladder cancer is the second most commonmalignancy of urologic tumors. Back in 1976, lasers were
added to the endourological armetarium for bladder tumortreatment. Despite nowadays’ standard procedure for staging and treating non-muscle invasive bladder tumor bytransurethral resection of bladder tumors (TURB) via a wire loop, laser resection techniques for bladder tumorcame back in focus with the introduction of Ho:YAG and not to mention recently Tm:YAG lasers. This review aimsto display the current evidence for these techniques. Materials and methods Throughout April 2010, MEDLINEand the Cochrane central register of controlled trials were searched previously for the following terms: ‘‘Laser,resection, ablation, coagulation, Nd:YAG Neodym, HoYAG: Holmium, Tm:YAG Thulium and transitionalcarcinoma, bladder, intravesical.’’ Results Eleven articles on Ho:YAG and 7 on Tm:YAGwere identified. Searches by Cochrane online library resulted in no available manuscripts. Conclusion Today, Nd:YAG does not play any role intreatment of lower urinary tract transitional cell carcinoma. Ho:YAG and Tm:YAG seem to offer alternatives in thetreatment of bladder cancer, but still to prove their potential in larger prospective randomized controlled studies withlong-term follow-up. Future expectations will show whether en bloc resection of tumors are preferable to the traditional‘‘incise and scatter’’ resection technique, in which is contrary to all oncological surgical principles. For theprimary targets, here are within first-time clearance of disease, in addition to low in-fields and out-of-fieldsrecurrence rates. |
| Transurethral 2- m laser in the treatment of urethral stricture 【尿道狭窄】 | Feng Fu Guo · Hua Lu · Guang Jian Wang · Shan Feng Tan · Xiang Fei He · Jian Ming Wang · Hong Jun Liu · Wen Bin Zhu |
Objectives To evaluate the curative eYcacy of transurethral 2- m thulium laser urethrotomy in the treatment of
urethral stricture. Methods Two hundred and thirty-eight patients suVering from urethral stricture, all male, aged 47.3 (36–58), underwent transurethral 2- m thulium laser urethrotomy. The maximum Xow rate (MFR), the international prostatic symptom score (IPSS) and the quality of life (QoL) were measured before operation, immediately following the removal of the catheter, and 3 and 6 months postoperatively. Results The surgery was performed for all the patients with no rectum injury, urine leakage or massive blood loss. All the patients got free urination immediately following the catheter removal with the mean MFR improved from (3.2 § 0.3) ml/s preoperatively to (16.7 § 3.1) ml/s, which kept steady to (18.7 § 2.9) and (19.2 § 2.8) ml/s, respectively 3 and 6 months after operation. IPSS signiWcantly improved from 28.3 § 5.8 preoperatively to 7.1 § 1.9, 6.4 § 1.5 and 5.3 § 1.3, respectively when catheter removal and 3 and 6 months after operation. Also during the corresponding period, mean QoL improved from 5.4 § 1.1 to 1.1 § 0.3, 0.9 § 0.2 and 0.8 § 0.2. 195, patients got permanent uninterrupted urination without recurrence in the whole 6 months of follow-up. Forty-three patients got recurrence and seven patients encountered with incontinence 1–3 weeks (mean 13.8 days) after catheter removal, but they all got Wnal cure after periodic urethral dilatation and physical exercise. Conclusions Transurethral 2- m thulium laser is safe and eYcient in the treatment of urethral stricture. |
| Laser-Supported Partial Nephrectomy for Renal Cell Carcinoma 腎細胞癌に対するレーザ腎部分切除術 | Torsten Gruschwitz, Renate Stein, Jörg Schubert, and Heiko Wunderlich |
OBJECTIVES
The extirpation of peripherally seated renal tumors by partial nephrectomy is an established method. To decrease the disadvantages of vascular hilar clamping, we proved the use of a laser for partial nephrectomy. To date, this laser application has only been described in the animal model. METHODS With an exophytic position of the renal tumor, we successfully performed nephron-sparing surgery without clamping of the renal vessels in 5 patients. RESULTS Regular ultrasound monitoring showed no evidence of postoperative hemorrhage. The serum creatinine, hemoglobin, and hematocrit were nearly unaltered before and after surgery. CONCLUSIONS The results of our study have shown that laser-supported partial nephrectomy without clamping of the renal vessels, particular in carefully selected patients, is a safe alternative to classic partial nephrectomy.
目的 腎部分切除により、抹消にできた腎腫瘍を摘出する方法が、確立されております。血管肺門をクランプすることによる欠点を減らすために、腎部分切除にレーザを用いることを証明しました。現在のところ、このレーザの適用は、動物モデルにおいてのみ報告されています。
方法 腎腫瘍が腎臓の外側に増殖している患者のうち、私達は5名の患者において、腎血管をクランプすることなく、腎温存手術を行うことに成功しました。 結果 定期的な超音波モニタリングにおいて、術後出血を示す形跡はなく、手術前後の血清クレアチニン、ヘモグロビン、ヘマトクリット値に、ほとんど変化はありませんでした。 結論 私達の研究結果では、レーザによる腎部分切除は、慎重に選択した患者に対して、腎血管をクランプせずに適用可能であり、従来の腎部分切除に取って代わる安全な手技であることが示されました。 |
| Current evidence of transurethral Ho:YAG and Tm:YAG treatment of bladder cancer: update 2014 | Mario W. Kramer · Mathias Wolters · Hannes Cash · Stephan Jutzi · Florian Imkamp · Markus A. Kuczyk · Axel S. Merseburger · Thomas R. W. Herrmann |
Abstract: Introduction Bladder cancer (BC) represents a growing health care problem worldwide. In times of tight budgets and an aging society, new strategies for the transurethral treatment of BC are needed. Laser devices used for tumor vaporization and/or en bloc resection provide an alternative to parvenu strategies.
Materials and methods: Medline/Cochrane search was performed using following terms: bladder cancer, urothelial carcinoma, laser, en bloc, vaporization, photoablation, holmium, thulium, Ho:YAG, Tm:YAG, HoLRBT and TmLRBT. Last date of search was February 12, 2014. Results : Eighteen publications in English were identified including 800 patients (Ho:YAG = 652 patients and Tm:YAG = 148 patients). Data on en bloc resection techniques were presented in 10 publications, 7 publications provided data of tumor vaporization and one publication presented data on both. Level of evidence based on SIGN is mainly 3 (non-analytic studies); only three studies are level 2 (prospective case control studies). Tumor vaporization seems to be a promising alternative for the treatment of recurrent tumors in selected patients. It can be performed in an office-based approach without the needof general anesthesia. The use of photodynamic diagnostic might enhance surgical quality. The principle of en bloc resection should provide accurate staging in most cases; however, data on this important aspect are missing. Peri- and postoperative complications are scarce. Due to the nature of the energy source, bladder perforation caused by obturator nerve reflex is highly unlikely when using lasers. There is a trend toward decreased infield recurrence rates. Conclusions : Lasers are potentially useful alternatives to conventional TURBT, but systematical assessments using standardized classification systems and well-designed RCTs are needed to make results comparable. |
| Tm:YAG laser en bloc mucosectomy for accurate staging of primary bladder cancer: early experience | Mathias Wolters · Mario W. Kramer · Jan U. Becker · Matthias Christgen · Udo Nagele · Florian Imkamp · Martin Burchardt · Axel S. Merseburger · Markus A. Kuczyk · Thorsten Bach · Andreas J. Gross · Thomas R. W. Herrmann |
Abstract: Introduction Exact pathological staging of bladder cancer is crucial for determination of further treatment. One limiting factor is the surgical ‘incise and scatter’ technique that might contribute to tumour recurrence. En bloc resection
techniques are en emerging issue. We present initial results with Thulium:YAG (Tm:YAG) en bloc resection of bladder tumours for treatment and accurate staging of solitary transitional cell carcinoma of the bladder. Materials and methods: From June through October 2010, six patients were treated by TmLRBT (Thulium laser resection of bladder tumour). Inclusion criteria were solitary lesions, treatment naive patients and tumour localisation of the lower bladder wall and trigonum. En bloc resection was applied on all of the tumours. Two cold-cut biopsies from the tumour base were extracted. On Wve of the six patients, a re-resection was performed after 6 weeks. Results: Pathological evaluation revealed 1 patient with pTa G1, 2 patients with pTa G2 and 3 patients with pT1 G3. All of the resected specimens provided detrusor muscle, and all biopsies were positive for muscle cells. No intra-, perior post-operative complications were observed. Bladder irrigation was mandatory in only 50% of the patients. All patients were negative for residual TCC in re-resection 6 weeks after initial treatment. Conclusion TmLRBT has been proven safe and eVective for both, treatment and pathological staging of primary TCC of the bladder. Tm:YAG en bloc resection therefore could be an appropriate tool for accurate staging with possibly lower scattering potential for the assessment and treatment of patients with TCC. |
| Thulium:yttrium-aluminumegarnet Laser for En Bloc Resection of Bladder Cancer: Clinical and Histopathologic Advantages | Giovanni Muto, Devis Collura, Alessandro Giacobbe, Leonardo D’Urso, Gian Luca Muto, Andrea Demarchi, Sergio Coverlizza, and Emanuele Castelli |
OBJECTIVE: To determine whether thulium:yttrium-aluminum-garnet laser resection of bladder tumor
(TmLRBT) may offer advantages over classic resection. ATERIALS AND METHODS: From April 2011 to September 2012, 55 consecutive patients newly diagnosed with clinical stage T2 bladder cancer were enrolled in a prospective study on TmLRBT. Neoplasm was removed en bloc in all cases. When the tumor size was >3 cm, it was necessary to incise longitudinally and/or across the lesion and the bladder wall at its the base into 2 or more parts. All cases of nonemuscle-invasive bladder cancer underwent second look in 30-90 days. RESULTS: Pathology reported urothelial carcinoma with Ta low grade in 31 patients (56.4%), T1 high grade in 18 (32.7%), and T2 high grade in 6 (10.9%). Histopathologic evaluation showed that the bladder detrusor was provided in all cases. Hemostasis was excellent, and no postoperative hematuria was reported. In a case of T1 G3, endoscopic re-evaluation showed a focal infiltration of the bladder detrusor, so the patient underwent radical cystectomy. To date, with a mean follow-up of 16 months (range, 8-25), the recurrence rate in patients with superficial disease is 14.5%. All recurrences were outside the site of first resection, and there was no progression in tumor grade. CONCLUSION: TmLRBT is a simple method that seems to overcome the “incise and scatter” problem associated with traditional transurethral resection of bladder tumor. Our initial data on staging accuracy and reduction of the local recurrence rate are encouraging. |
| 文献名 | 著者 | アブストラクト |
| Hysteroscopic myomectomy using a two-micron continuous wave laser (RevoLix) 子宮筋腫摘出 | Ching-Hui Chen a, Wen-Ling Lee b,c,d,e, I-Te Wang a, f, Yuan-Kuei Yen a, f, Li-Hsuan Chiu a, Chii-Ruey Tzeng a, f, Wei-Min Liu a, f,* |
jectives: The safety and efficacy of the RevoLix 2-m continuous wave laser for hysteroscopic myomectomy
(HM) was evaluated. Materials and methods: A retrospective study was undertaken to evaluate 13 patients with symptomatic submucous myomas, who were treated with HM using a RevoLix laser application. The evaluation items included blood loss from surgery (estimated by the change between preoperative and postoperative hemoglobin levels), surgical time, amount of distension media, specimen volume retrieved, complications, and success rate. Results: The mean age of the patients was 38 years old; 10 patients were in the premenopausal status and nine patients were nullipara. The surgical time was 91 minutes, and the distension media requirement was 4500 mL. The postoperative hemoglobin level decreased to 1.2 g/dL compared with the preoperative status. Mean specimen volume retrieved was 13.7 mm. No complications occurred. All patients reported significant improvement after HM during the 1-year follow-up. Conclusion: The use of the Revolix laser for HM seemed to be safe and effective in the management of symptomatic submucous myomas in this small population study. |
| 2μm 連続波ツリウムレーザでの口腔扁平上皮癌切除は病理検査に悪影響なし | Ajit J. Pothen, MD,1_ Januska Evenboer, MD,1 Justin E. Swartz, BSC,1 Stefan M. Willems, MD, PhD,2 Ellen M. Van Cann, MD, PhD,3 Luuk M. Janssen, MD, PhD,1 Geert J. van der Heijden, PhD,1,4 and Wilko Grolman, MD, PhD1 |
背景と目的:現在行われている口腔扁平上皮癌(OSCC)の切除方法は、スチール製のメス から炭酸レーザ、モノポーラの電気メス(MO)まで多種に及びます。私達は病理検査につ いて、新しい治療法のツリウムレーザ(TL)と MO を比較しました。
研究計画 / 対象患者および方法:TL または MO を受けた OSCC 患者 42 人を対象としま した。切除縁(安全域)解釈と熱損傷に特に注目して、切除検体をすべて評価しました。 結果:熱損傷深度範囲は病理検査を妨げることなく、MO グループの 1.0~4.0mm に対し、 TL グループでは 1.0~3.5mm でした。切除縁陽性の割合は、MO グループの方が多く、TL グループの 3 倍という結果でした。 結論:本研究は、MO切除と比較し、TL切除が病理検査を妨げるものではないことを示し ています。Lasers Surg. Med. 9999:XX–XX, 2014. ⓒ 2014 Wiley Periodicals, Inc. |
| 腎細胞癌に対するレーザ腎部分切除術 | Torsten Gruschwitz, Renate Stein, Jörg Schubert, and Heiko Wunderlich |
目的:腎部分切除により、末梢にできた腎腫瘍を摘出する方法が、確立されております。血管腎門をクランプすることによる欠点を減らすために、腎部分切除にレーザを用いることを証明しました。現在のところ、このレーザの適用は、動物モデルにおいてのみ報告されています。
方法:腎腫瘍が腎臓の外側に増殖している患者のうち、私達は5名の患者において、腎血管をクランプすることなく、腎温存手術を行うことに成功しました。 結果:定期的な超音波モニタリングにおいて、術後出血を示す形跡はなく、手術前後の血清クレアチニン、ヘモグロビン、ヘマトクリット値に、ほとんど変化はありませんでした。 結論:私達の研究結果では、レーザによる腎部分切除は、慎重に選択した患者に対して、腎血管をクランプせずに適用可能であり、従来の腎部分切除に取って代わる安全な手技であることが示されました。 |
| Laser-supported partial laparoscopic nephrectomy for renal cell carcinoma without ischaemia time 【腎癌治療における腎部分切除(ヒトへの摘要11人)虚血時間を短くする試み】 | Hagen Loertzer*, Arne Strauß, Rolf Herrmann Ringert and Philine Schneider |
Background: To date, elective nephron-sparing surgery is an established method for the exstirpation of renal
tumors. While open partial nephrectomy remains the reference standard of the management of renal masses, laparoscopic partial nephrectomy (LPN) continues to evolve. Conventional techniques include clamping the renal vessels risking ischaemic damage of the clamped organ. Thus, new techniques are needed that combine a sufficient tissue incision for exstirpation of the tumor with an efficient coagulation to assure haemostasis and abandon renal vessel clamping in LPN. Laser-excision of renal tumors during laparoscopic surgery seems to be a logical solution. Methods: We performed nephron-sparing surgery without clamping of the renal vessels in 11 patients with a renal tumor in exophytic position (mean size 32 mm, ranging 8–45 mm) by laser-supported LPN. Results: Regular ultrasound monitoring and insertion of a temporary drainage showed no evidence of postoperative hemorrhage. All tumors were removed with a histopathologically confirmed surrounding margin of normal renal tissue (R0 resection). Serum creatinine, hemoglobin, and hematocrit were nearly unaltered before and after surgery. Conclusions: The experience won in these patients have confirmed that laser-assisted LPN without clamping of the renal vessels could be a safe and gentle alternative to classic partial nephrectomy in patients with exophytic position of renal tumors. |
| Use of the 2-mm Continuous Wave Thulium Laser for the Resection of Oral Squamous Cell Carcinomas does not Impair Pathological Assessment 【口腔扁平上皮癌】 | Ajit J. Pothen, MD,1 Januska Evenboer, MD,1 Justin E. Swartz, BSC,1 Stefan M. Willems, MD, PhD,2 Ellen M. Van Cann, MD, PhD,3 Luuk M. Janssen, MD, PhD,1 Geert J. van der Heijden, PhD,1,4 and Wilko Grolman, MD, PhD 1" |
Background and Objective: Current resection modalities for oral squamous cell carcinomas (OSCC) vary from
cold steel over CO2 laser to monopolar electro-surgery (MO). We compared thulium laser (TL) as a new modality with MO with regards to pathological assessment.Study Design/Materials and Methods: Forty-two patients who were treated for OSCC by either TL or MO were included. All resected specimens were assessed with special attention to margin interpretation and thermal damage. Results: Depth of thermal damage ranged from 1.0 to 3.5mmin the TL group compared to 1.0–4.0mmin theMO group without interfering with the pathological assessment.The percentage of positive margin resections was three times higher in the MO group compared with the TL group. Conclusions: This study shows resections done by TL donot impair pathological assessment when compared to MO resections. Lasers Surg. Med. 9999:XX–XX, 2014. |
| Clinical feasibility trial on 1940 nm Tm: fiber laser intervention of hyperplastic inferior nasal turbinates 【下鼻甲介の肥厚】 | Ronald Sroka*, Miriam Havel, Christian Betz, Thomas Kremser and Andreas Leunig |
Introduction: A number of different laser systems have been used for volume reduction of hyperplastic nasal tur- binates. In case of endonasal application, fiber-controlled diode lasers are preferred due to reasons of cost and prac- ticability. The aim of this clinical feasibility study was to show the coagulative and tissue reducing effects using a novel Tm: fiber laser system emitting at λ=1940 nm.
Patients and methods: This clinical feasibility trial included 11 patients suffering from hyperplastic inferior nasal turbinates, who were therapy-refractory to conser- vative medical treatment. The obstructive nasal cavity was treated using the 1940 nm Tm: fiber laser at <5 W output power. The treatment was performed in non-contact mode under endoscopic control. Patients’ symptoms were documented both preoperatively and on days 1–3 and 28 postoperatively using a non-validated questionnaire. Additionally, an endoscopic examination was performed. Results: None of the patients showed infections, and no hem- orrhages or other complications occurred intra- or postop- eratively. The mean laser activation time during the surgical procedure was extremely short being 28.08.5 s. In conjunc- tion with a low power setting (median, 3 W; meanstand- ard deviation, 3.31.1 W), a low energy of 90.237.8 J was applied. A significant reduction in nasal obstruction could be documented in all patients on day 28 postoperatively. Evaluation, as assessed preoperatively and 4 weeks postop- eratively, showed significant subjective improvements. Conclusion: The treatment of hyperplastic inferior turbi- nates using a 1940 nm Tm: fiber laser provides sufficient tissue reduction in a short operation time using low total energy. Patients described a significant improvement in nasal breathing postoperatively. |
| Office-based laryngeal laser surgery: A review of 443 cases using three wavelengths 【再発性呼吸器乳頭腫症、声門形成異常、声帯肉芽腫、バレット食道、ラインケ浮腫、喉頭アミロイド症など】 | Jamie A. Koufman, MD, Catherine J. Rees, MD, William D. Frazier, MD, Lauren A. Kilpatrick, BS, S. Carter Wright, MD, Stacey L. Halum, MD, and Gregory N. Postma, MD, New York, NY; Sacramento, CA; Winston-Salem, NC; Indianapolis, IN; Augusta, GA |
BACKGROUND: Unsedated office-based laser surgery (UOLS) of the larynx and trachea has significantly improved the treatment options for patients with laryngotracheal pathology including recurrent respiratory papillomas, granulomas, leukoplakia, and polypoid degeneration. UOLS delivered by flexible endoscopes has dramatically impacted office-based surgery by reducing the time,costs, and morbidity of surgery.
OBJECTIVES: To review our experience with 443 laryngotracheal cases treated by UOLS. METHODS: The laser logbooks at the Center for Voice and Swallowing Disorders were reviewed for UOLS, and the medical and laryngological histories were detailed, as were the treatment modalities, frequencies, and complications. RESULTS: Of the 443 cases, 406 were performed with the pulsed-dye laser, 10 with the carbon-dioxide laser, and 27 with the thulium: yttrium-aluminum-garnet laser. There were no significant complications in this series. A review of indications and waveleng thselection criteria is presented. CONCLUSION: Unsedated, office-based, upper aerodigestive tract laser surgery appears to be a safe and effective treatment option for many patients with laryngotracheal pathology. © 2007 American Academy of Otolaryngology–Head and Neck Surgery Foundation. All rights reserved. |
| Thulium laser in airway diseases in children 【小児の気道】 | Sonia Ayari-Khalfallah, Carine Fuchsmann and Patrick Froehlich |
Purpose of review
To specify the characteristics of the thulium laser and to evaluate the advantages and possibilities of treatment with this laser in laryngotracheal diseases in children. Recent findings Fiber-based lasers have facilitated a new style of surgery. When performing therapeutic airways endoscopies there is the possibility of good control of lesions and adequate visualization of the surgical field using the telescope. Different types of laser may be used but the 2013-nm thulium laser shows promise as a laser that is efficient in soft tissues with the advantages of the other lasers without their problems. The thulium laser has been described in treating urinary tract abnormalities and recently airways diseases in adults, but there are no reports of other uses for this technique in the pediatric airway. Summary The thulium laser appears to be an interesting tool in the management of laryngotracheal diseases such as subglottic stenosis, tracheal granuloma and laryngomalacia. The use of this laser in laryngotracheal diseases in children will probably progress in the future. |
| Office-Based and Microlaryngeal Applications of a Fiber-Based Thulium Laser 【声門(癌、アミロイド症、肉腫、血管腫、乳頭症)】 | Steven M. Zeitels, MD; James A. Burns, MD; Lee M. Akst, MD; Robert E. Hillman, PhD; Matthew S. Broadhurst, MD; R. Rox Anderson, MD |
Objectives: The carbon dioxide {CO2) laser is the premier dissecting instiutnent for hemostatic cutting and ablation during
endolaryngeal surgery. However, microlaryngeal tangential dissection and office-based photoablation have been limited by the lack of a fiber-based delivery system. To address this limitation, a new laser was designed, which is a diodepumped solid-state laser with a ihtilitim-doped yttrium-aliiminiim-garnet laser rod. It produces a continuous-wave beam with a wavelength of 2,013 nm and a target chromophore of water. This new laser functions similarly to a CO2 laser with the benefit of being delivered through a small glass fiber (0.365 to 0.550 tnm). Methods: A prospective pilot trial was done in 74 cases to explore applications of the new thulium laser. Thirty-two procedures were done with the laser used as an ablating instrument and topical anesthesia through a flexible laryngoscope {papillomatosis,20: microinvasive carcinoma. 6; benign supraglottic lesions. 3: edema. 2; granuloma. 1). Forty-two procedures were done with the laser used as a cutting or ablating instrument for microlaryngeal dissection and general anesthesia. These included 27 partial laryngeal resections (supraglottis. 15: glottis. 10: subglottis. 2) and 8 posterior giottic laryngoplasties. The laser was al.so used as an ablative instrument during microlaryngoscopy in 7 cases. Results: The thulium laser was used effectively in all cases, under both local and general anesthesia. In microlaryngeal dissection, electrocautery was not needed to control bleeding.even during cutting in the highly vascular paraglottic space. No compiications related to the use ofthe thulium laser were experienced in any case. Conclu-sions: Because ofthe fiber-based delivery system, the 2.013-nm continuous-wave thulium laser shows substantial promise for tangential dissection during mierolaryngoscopy and soft tissue photoablation during office-based flexible laryngoscopy. Hemostasis was judged to be superior to experiences with the CO: laser. In this pilot study, performing en bloc laryngeal cancer resection procedures was facilitated by use ofthe thulium laser. |
| Clinical Study on Climacteric Dysfunctional Uterine Bleeding Treated with RevoLix 2 Micron Continuous Wave Laser Vaporesection and Hysteroscopic Endometrial Electroresection 【閉経後の子宮不正出血】 | MEI Songyuan,SUN Xiaobo,LIU Guizhi,et al |
Objective:To explore the clinical curative effect of RevoLix 2 micron continuous wave laser vaporesection in treatment of patients with cli macteric dysfunctional uterine bleeding.Methods:26 patients with climacteric dysfunctional uterine bleeding who were treated with RevoLix 2 micron continuous wave laser vaporesection were selected as observation group,and 26 patients with climacteric dysfunctional uterine bleed ing who were treated with hysteroscopic endometrial electroresection were selected as control group,the operation times,the amounts of blood loss during operation and clinical curative effects in the two groups were compared.
Results:The operation time in observation group((16.9±4.5)minutes)was significantly longer than that in control group((13.9±3.8)minutes)(P0.05).The amount of blood loss during operationin observation group((10.6±3.5)mL)was fewer than that in control group((14.2±4.2)mL)(P0.05).The total effective rates in observation group and control group were 92.3% and 96.2%,respectively,there was no significant difference between the two groups(P0.05) .Conclusions:The clinical curative effect of RevoLix 2 micron continuous wave laser vaporesection is good in treatment of patients with climacteric dysfunctional uterine bleeding,the complications are few,which is a safe,simple and effective method.Further studies are necessary to evaluate its long-term effect. |
| 腎細胞癌に 対する 虚血時間を 虚血時間を なくしたレーザによる レーザによる 腹腔鏡下腎部分切除 | Hagen Loertzer*, Arne Straus, Rolf Herrmann Ringert and Philine Schneider |
要約
背景:現在のところ、選択的腎温存手術が、腎腫瘍を摘出する方法として確立されています。開腹腎部分切除が腎腫瘤を管理する参考基準となっている一方で、腹腔鏡下腎部分摘除術(LPN)が進化しています。従来の方法では、腎血管をクランプするため、クランプした臓器が虚血性障害となるリスクがあったため、新しいLPNでは、腫瘍を摘出するための十分な組織切開と、止血を確実にし、腎血管クランプを不要にする効率的な組織凝固を兼ね備えた技術が必要とされます。レーザによる腹腔鏡下腎腫瘍切除は、論理的解決法と考えられています。 方法:腎腫瘍(平均サイズ32mm、範囲8~45mm)が腎臓の外側に増殖している患者11名に対して、腎血管をクランプすることなく、レーザによるLPNで、腎温存手術を実施しました。 結果:定期的な超音波診断、および一時的に挿入したドレナージカテーテルにおいて、術後の出血を示す形跡はありませんでした。すべての腫瘍は、病理組織学的に確認された周囲の正常な腎組織の辺縁ごと摘出しました(R0切除)。血清クレアチニン、ヘモグロビン、ヘマトクリット値は、手術前後で、ほとんど変化はありませんでした。 結論:今回の研究結果を通して、レーザによるLPNは、腎腫瘍が腎臓の外側に増殖している患者に対して、腎血管をクランプせずに適用可能であり、従来の腎部分切除を代替する安全で低侵襲な治療法となり得ることが確認されました。 キーワード:レーザ腎部分切除、腹腔鏡下腎部分切除、虚血なしの腎切除、虚血、レーザ |
| 2μm 連続波ツリウムレーザでの口腔扁平上皮癌切除は 病理検査に悪影響なし | Ajit J. Pothen, MD,1_ Januska Evenboer, MD,1 Justin E. Swartz, BSC,1 Stefan M. Willems, MD, PhD,2 Ellen M. Van Cann, MD, PhD,3 Luuk M. Janssen, MD, PhD,1 Geert J. van der Heijden, PhD,1,4 and Wilko Grolman, MD, PhD1 |
背景と目的:
現在行われている口腔扁平上皮癌(OSCC)の切除方法は、スチール製のメス から炭酸レーザ、モノポーラの電気メス(MO)まで多種に及びます。私達は病理検査につ いて、新しい治療法のツリウムレーザ(TL)とMO を比較しました。 研究計画 / 対象患者および方法:TL またはMO を受けたOSCC 患者42 人を対象としました。切除縁(安全域)解釈と熱損傷に特に注目して、切除検体をすべて評価しました。 結果: 熱損傷深度範囲は病理検査を妨げることなく、MO グループの1.0~4.0mm に対し、TL グループでは1.0~3.5mm でした。切除縁陽性の割合は、MO グループの方が多く、TLグループの3 倍という結果でした。 結論: 本研究は、MO切除と比較し、TL切除が病理検査を妨げるものではないことを示しています。 |
| 前立腺肥大症に対するツリウムレーザー蒸散術および核出術の検討. | 小泉充之, 中島健寛, 西村玲応奈, 深澤佳高, 藤川敦 横須賀市立市民病院泌尿器科 |
要旨:2016年11月から2017年8月までの間に施行したツリウムレーザー
前立腺蒸散術(ThuVAP)27例、計85例を対象に後ろ向き検討を行った。 術前評価と術後1-3ヶ月の間に行った短期的評価の比較では、IPSS, QOLスコア、 最大尿流率、および残尿量は、中央値においていずれも有意な改善を認めた。術後合併症については、 重度の出血や前立腺被膜の穿孔や膀胱穿孔等の重篤なものは認めなかった。今回、短期の評価において、 ThuVAP・ThuLEPとともに比較的安全であり、排尿機能は術直後から改善された。ツリウムレーザーは 前立腺肥大症に対する術において有用であると考えられた。 |
| ツリウムレーザーを用いた経尿道的内視鏡手術:現状と新たな展開 | 小路 直* 大瀧達也 宮嶋 哲 |
"要旨 前立腺肥大症 (Benign Prostatic Hyperplasia, 以下BPH) に対するツリウムレーザー手術は, 2015年にわが国に導入され, 2017年には男性下部尿路症状・前立腺肥大症診療ガイドラインでは, 治療の効果と安全性においてエビデンスレベル2, 治療は推奨グレードBとして示されている. ツリウムレーザーは, 出血の少ない切開, 出力エネルギーに応じた蒸散が可能であるため, 経尿道的前立腺核出術, および蒸散術のモダリティーとして世界的に使用されている. ツリウムレーザーの波長は 1,940-2,013 nmであり, 水分子に吸収されやすく, 前立腺組織への深達長は, 0.2 mmと浅い. また, 連続波モードでの照射が可能であるため, 連続照射による高い蒸散, 凝固能力と切開能を併せ持つレーザーとして, BPHに対する治療として普及している. ツリウムレーザーを用いたBPHの治療として, 高い凝固能と切開能を活かしたツリウムレーザー前立腺核出術 (Thulium laser enucleation of the prostate, 以下ThuLEP), 安定したレーザー深達長による安全性の高い蒸散能を活かしたツリウムレーザー前立腺蒸散術 (Thulium laser vaporization of the prostate, 以下ThuVAP) が行われている. 特にThuLEPは, 無作為化比較試験において他術式と比較して出血量が少なく, 短いカテーテル留置期間が得られる治療であることが示されている. また, ツリウムレーザーは出血のリスクの高い他科領域での手術における有用性も報告されていることから, 複数診療科でのニーズがあるレーザーとして今後の普及が期待される.
Key words 前立腺肥大症, ツリウムレーザー, 内視鏡手術, 核出術, 蒸散術" |
| Tm: YAG レーザーを用いた前立腺肥大症の治療 | 小路 直 (東海大学医学部付属八王子病院泌尿器科准教授) |
"ツリウムレーザーの波長は2013nmであり,水分子に吸収されやすく,組織への影響は深さ1mm未満と少ない特性を持つ。また,凝固能,切開能および蒸散能を併せ持つレーザーとして,多くの外科的手術領域において期待されている。 ツリウムレーザー前立腺核出術(ThuLEP)は,内腺と外腺の間を剝離,核出する際にツリウムレーザーの特長を用いる術式である。前立腺肥大症に対する他の術式との前向き無作為化比較試験では,本術式の少ない出血量,短い入院期間および性機能への低侵襲性が示されてきた。
筆者らは,2015年11月にわが国で初めて,RevoLixTM(LISA laser products OHG,Germany)を用いたThuLEPを導入した。術後6カ月間以上経過観察可能であった30症例の年齢中央値は75歳,前立腺体積中央値は53mL,核出切除量中央値は30g,レーザー照射時間中央値は17分間,術後カテーテル留置期間中央値は2日間であった。合併症として重篤なものはなく,輸血は必要としなかった。術前,術後3カ月目,6カ月目における排尿機能に関する質問票(国際前立腺症状スコア,過活動膀胱症状スコア)および尿流量測定検査では,術前と比較してすべての項目で有意な改善が認められ,性機能への明らかな影響は認められなかった1)。 ツリウムレーザーは,抗凝固薬内服中の患者に対しても安全に使用可能という報告があり,本術式は,抗凝固薬を中止できない前立腺肥大症に対して実施可能な根治的治療法として期待されている。 Key Words Tm: YAG レーザー、肥大症、核出術、切除、蒸散" |
| 前立腺肥大症に対する Thulium laser 前立腺核出術 (ThuLEP) vs. TUR-P: 無作為化比較試験の現状 | 小路 直, 武田 和真, 内田 貴人, 杠 総一郎, 花田 いずみ, 黒田 悟史, 小川 貴博, 日暮 太朗, 中野 まゆら, 川上 正能, 新田 正広, 長谷川 政徳, 河村 好章, 宮嶋 哲 |
【目的】BPHに対するThuLEPとBipolar TUR-Pの比較試験の現状を報告する. 【対象と方法】対象は,
BPHに対して手術療法が必要となった症例. ThuLEP群およびTUR-P群を比較した. 【結果】ThuLEP群 (n=55) およびTUR-P群 (n=55) において, 排尿状態は, 術後に有意な改善が認められた. 一方, ThuLEP群は術前後のHb減少量が少なく (P=0.032), カテーテル留置期間は短期間であった (P=0.048). また, ThuLEP群では, 術後3カ月目以上に勃起機能の回復が認められた. 【考察】ThuLEP およびTUR-P群ともに治療効果は同等であったが, 止血, カテーテル留置期間, および勃起温存に おいて, ThuLEPの有用性が示唆された. Key Words: 前立腺肥大症, ツリウムレーザー, 経尿道的前立腺切除術, 排尿機能, 性機能 |
奥野 紀彦 先生
独立行政法人国立病院機構相模原病院
小路 直 先生 東海大学医学部外科学系泌尿器科学
BPH動画
BPH動画
BPH動画
BPH動画
BPH動画
BPH動画
BPH動画
口腔外科
口腔外科
口腔外科
口腔外科
口腔外科
口腔外科
口腔外科
口腔外科
腎部分切除
腎部分切除
尿管狭窄
膀胱癌切除
膀胱癌切除
Specialty: The pioneer Laser Urology , Gynecology, ENT surgical technique

The Revolix Thulium laser is the only laser system developed especially for soft tissue surgery. The wavelength of the Revolix laser is 2 microns. This wavelength is absorbed by any tissue by the ubiquitous water molecule.
The Revolix wavelength is similar to the Holmium but the emission mode is continuous instead of pulsed, so the Revolix offers a continuous vaporization effect instead of tearing tissue like the Holmium laser.
The strong tissue absorption of the Revolix wavelength, in any irrigation fluid and water, provides an immediate effect on the tissue, limited penetration, excellent hemostasis and protection against collateral damage.
Revolix combines the benefits of laser surgery in a single device.
The 2.0 micron wavelength of the RevoLix is excellent for incision and ablation. It is safe in water irrigation and provides excellent homeostasis. The effect of the laser on the tissue is independent of the vascularization of the tissue.
These properties are due to the efficient absorption effect of the 2.0 micron wavelength by the water molecule, which is omnipresent in any tissue.
Strong absorption and continuous wave emissions provide perfect cuts and soft tissue vaporization with excellent homeostasis. There is no deep penetration or uncontrolled necrosis. Clean cuts and excellent homeostasis are achieved by moving the fiber along the surgical site.
Its incomparable power allows rapid resection or vaporization of large volumes of tissue. Its speed of section and its quality of hemostasis is superior to any known alternative.
In an aqueous irrigation the effect of the laser on the tissue is restricted to less than 3 mm from the front of the fiber tip. All the most distant tissue is protected by the aqueous solution. The same mechanism protects the tissue and organs adjacent to the cut. Any fabric over a distance of more than 3 mm is not affected by the RevoLix laser. This property eliminates the risk of unintentional tissue damage during laser surgery. Combined with suitable accessories and fibers, the RevoLix leaves the practitioner the choice of his operating technique in the treatment of prostate pathologies:
RevoLix offers a variety of HBP options:
For RevoLix there is no limitation on the size of the prostate. Gland volumes of up to 200 ml can be treated. Approximately 1.5 grams of tissue per minute are enucleated.
RevoLix is extremely easy to use, operates quietly and the wide wheels allow it to be transported between different rooms. Revolix can be plugged into any standard electrical outlet. RevoLix has been proving its durability during routine transport between different infrastructures and use by mobile healthcare units.
2 different RevoLix models are available. The 120 watt model ideal for enucleation of the prostate and the 200 watt model, which has tissue vaporization increased to more than 3g per minute. Fabric damage is the same on all RevoLix models
The optional Kix DUO Dual Pedal allows you to switch between cutting and coagulation settings or to control the cutting speed, faster or slower. The single Pedal is also available.
TOP